 |
Clinical Image
A rare case of pemphigus vegetans with underlying diffuse large B-cell lymphoma
1 MD, Department of Internal Medicine, St. Luke’s University Health Network, Bethlehem, PA, United States
2 MD, Department of Internal Medicine, St Mary Medical Center, Langhorne, PA, United States
3 DO, Department of Hematology & Oncology, St. Luke’s University Health Network, Bethlehem, PA, United States
4 MD, Medical Director of Genitourinary Cancer Program, St. Luke’s University Health Network, Bethlehem, PA, United States
Address correspondence to:
Aashima Gupta
MD, 801 Ostrum Street, Bethlehem, PA,
United States
Message to Corresponding Author
Article ID: 100155Z10AG2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Gupta A, Kelley MA, Schmoyer J, Arriaga Y. A rare case of pemphigus vegetans with underlying diffuse large B-cell lymphoma. J Case Rep Images Oncology 2026;12(1):14–16.ABSTRACT
No Abstract
Keywords: DLBCL, Lymphoma, Paraneoplastic syndrome, Pemphigus vegetans
Case Report
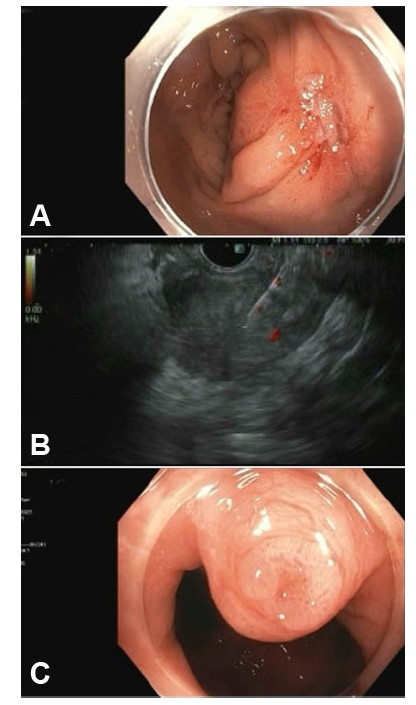
A 72-year-old female presented in 2022 with small bowel obstruction caused by a small bowel mass. She underwent surgical resection of the mass, with pathology showing Diffuse Large B-Cell Lymphoma (DLBCL), of the small intestine. She declined systemic therapy for DLBCL and initiated surveillance. In 2025, she was admitted to the hospital with a 5-month history of enlarging, painful skin lesions on her intertriginous areas and toes in the setting of new lymphadenopathy, more noticeable in her right axilla.
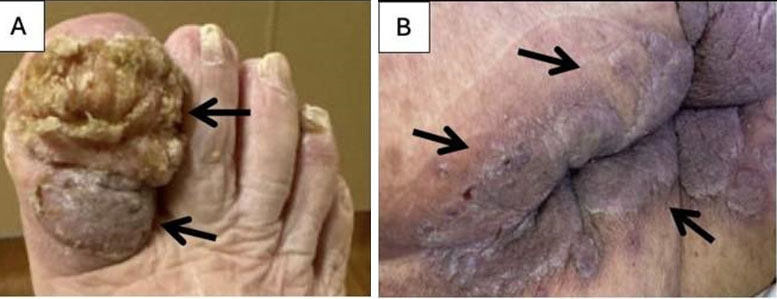
Her skin examination showed exophytic lesions on her toes and diffuse hyperpigmented verrucous plaques with crusting, involving intertriginous areas (Figure 1). The Nikolsky sign was negative and no mucosal involvement noted. Laboratory blood work was unremarkable except for a mildly elevated serum LDH of 291 U/L (Normal 122–222 U/L). Fluorodeoxyglucose (FDG)PET/CT scan demonstrated new FDG-avid uptake in a large right-sided axillary mass, lymph nodes in the right upper neck and bilateral pelvic region. In addition, there was extensive skin thickening.
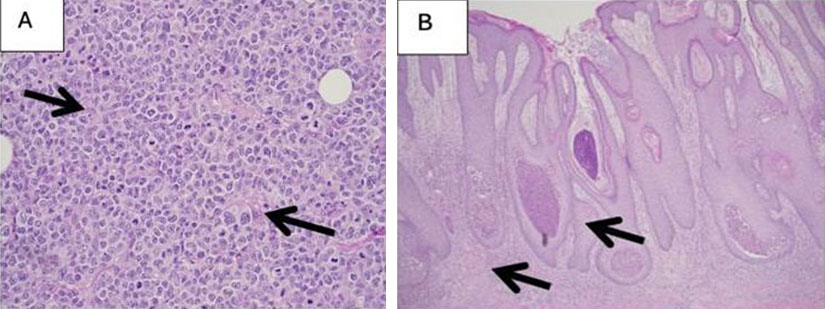
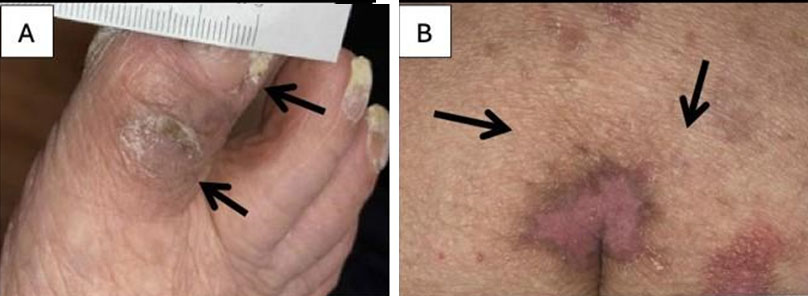
Subsequently, the patient underwent excisional biopsy of the right axillary lymph node, which confirmed a diagnosis of DLBCL recurrence with immunohistochemistry staining showed positive for CD20, CD10, BLC-6, MUM-1, cMYC, p53. The stains were negative for BCL-2, CD30, AE 1/3, CAM5.2, and CD23 (Figure 2A). The Ki67 index was 70–80%. Fluorescence in situ hybridization (FISH) analysis did not show any translocations of BCL-2, BCL-2, or MYC. Biopsy of a breast skin fold plaque showed pemphigus vegetans (PV) (Figure 2B). Serologic positivity for anti-desmoglein 3 and desmoglein 1 antibodies further supported a diagnosis of PV. The patient was treated with 6 cycles of rituximab, cyclophosphamide, vincristine, doxorubicin, and prednisone. After completion of 6 cycles of systemic therapy, she achieved remission of DLBCL and had resolution of all PV lesions (Figure 3).
Discussion
Pemphigus vegetans (PV) is one of the rarest variants of pemphigus, reported for only 1–2% of all pemphigus cases, which makes its diagnosis particularly challenging [1]. It classically presents with vegetative plaques involving intertriginous areas and the oral mucosa. Our patient presented with an atypical presentation, where, in addition to intertriginous verrucous lesions, she developed an exophytic/fungating lesion of the toe, a site not commonly reported in the literature.
The pathophysiology of PV involves autoantibodies directed against desmoglein (Dsg) 3 and/or desmoglein (Dsg) 1, disrupting epidermal adhesion and leading to the characteristic clinical findings. The association between PV and diffuse large B-cell lymphoma (DLBCL) has been reported in only a handful of cases, and whether DLBCL acts as a triggering factor for PV remains unclear. In our patient, DLBCL recurrence was identified concurrently with the diagnosis of PV. This temporal relationship raises the question of whether the two conditions share a pathological link either as a coincidental autoimmune process or as a paraneoplastic manifestation.
Diagnosis of PV is based on a combination of clinical features, histopathologic findings, and serologic evidence of antibodies against Dsg1 and/or Dsg3, confirmed by direct or indirect immunofluorescence [2],[3]. Our patient met the diagnostic criteria for classic PV. The temporal correlation between DLBCL recurrence and the eruption of PV lesions further strengthens the argument for an association between the two conditions.
Treatment of PV typically involves immunosuppressive agents, including corticosteroids, cyclophosphamide, azathioprine, dapsone, and mycophenolate, among others [4],[5],[6]. Given the potential association between DLBCL and PV in our patient, we pursued a unified treatment strategy using the R-CHOP regimen (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) to target the underlying lymphoma. The patient demonstrated a favorable response, with clearance of lesions in the intertriginous regions and the toe, lending further support to the hypothesis of a paraneoplastic relationship.
This case presents a rare and instructive co-occurrence of PV and DLBCL recurrence. Although the patient met diagnostic criteria for PV, the clinical response to lymphoma-directed therapy suggests a meaningful underlying association. This case underscores the importance of recognizing atypical cutaneous presentations and rare pemphigus variants as potential indicators of an occult or recurrent hematological malignancy—a recognition that may significantly inform and streamline the treatment approach.
Conclusion
The paraneoplastic association of PV with lymphoproliferative disorders is exceedingly rare, and it has been limited to case reports in the literature. The purpose of the current case report is to recognize the clinical association between lymphoproliferative disorders and PV. Clinicians evaluating patients with PV without known malignancy should consider an underlying lymphoproliferative disorder as a plausible association with PV. The presence of PV may serve as a clinical clue for the early identification of a lymphoproliferative disorder. Timely management of the primary lymphoproliferative disorder or underlying malignancy remains the foundation for PV resolution, avoiding delays in initiation of appropriate therapy and improving clinical outcomes.
REFERENCES
1.
von Köckritz A, Ständer S, Zeidler C, Metze D, Luger T, Bonsmann G. Successful monotherapy of pemphigus vegetans with minocycline and nicotinamide. J Eur Acad Dermatol Venereol 2017;31(1):85–88. [CrossRef]
[Pubmed]

2.
Mergler R, Kerstan A, Schmidt E, Goebeler M, Benoit S. Atypical clinical and serological manifestation of pemphigus vegetans: A case report and review of the literature. Case Rep Dermatol 2017;9(1):121–30. [CrossRef]
[Pubmed]
3.
Zaraa I, Sellami A, Bouguerra C, Sellami MK, Chelly I, Zitouna M, et al. Pemphigus vegetans: A clinical, histological, immunopathological and prognostic study. J Eur Acad Dermatol Venereol 2011;25(10):1160–7. [CrossRef]
[Pubmed]
4.
Ruocco V, Ruocco E, Caccavale S, Gambardella A, Lo Schiavo A. Pemphigus vegetans of the folds (intertriginous areas). Clin Dermatol 2015;33(4):471–6. [CrossRef]
[Pubmed]
5.
Sawai T, Kitazawa K, Danno K, Sugie N, Machizuki T, Sugiura H, et al. Pemphigus vegetans with oesophageal involvement: Successful treatment with minocycline and nicotinamide. Br J Dermatol 1995;132(4):668–70. [CrossRef]
[Pubmed]
6.
Tavakolpour S. Current and future treatment options for pemphigus: Is it time to move towards more effective treatments? Int Immunopharmacol 2017;53:133–42. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
- The authors thank Antonio Serrano, MD for assistance in obtaining pathological images and providing descriptions.
- The authors used Claude 3.5 Sonnet for linguistic refinement and structural editing of this manuscript. The final content and clinical interpretations remain the sole responsibility of the authors.
Aashima Gupta - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Maria A Kelley - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jeremy Schmoyer - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yull Arriaga - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Aashima Gupta et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}