 |
Case Report
Aggressive PTH-secreting lung carcinoma with a BRD3: NUTM1 fusion presenting with refractory hypercalcemia
1 Resident Doctor, Guy’s and St Thomas’ NHS Foundation Trust, Medical Oncology, London, United Kingdom
2 Department of Histopathology, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom
3 Respiratory consultant, University Hospital of Lewisham, Lewisham High Street, London, United Kingdom
4 Oncology consultant, Cancer Centre at Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom; School of Cancer and Pharmaceutical Sciences, King’s College London, Guy’s Campus, Great Maze Pond, London, United Kingdom
5 Oncology consultant, Cancer Centre at Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom
Address correspondence to:
Rosa Evans
St Thomas Hospital, Westminster Bridge Road, London SE1 7EH,
United Kingdom
Message to Corresponding Author
Article ID: 100148Z10RE2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Evans R, Abbotts K, Mclean E, Simpson T, Georgiou A, Gennatas S. Aggressive PTH-secreting lung carcinoma with a BRD3: NUTM1 fusion presenting with refractory hypercalcemia. J Case Rep Images Oncology 2025;11(2):6–10.ABSTRACT
Introduction: Nuclear protein in testis (NUT) midline carcinomas (NMCs) are rare and aggressive cancers. These carcinomas are defined by gene re-arrangement leading to fusion of the NUT gene on chromosome 15 with other genes. These are named as such as they are solid tumors most frequently occurring in the midline including lung, central nervous system, kidneys, head and neck. They are underdiagnosed and under-reported, with most available literature on them in the form of case reports and case series. There are currently no targeted treatments available, and as a result they are associated with poor outcomes. We report an unusual case of this cancer type: a BRD3::NUTM1 fusion lung cancer presenting with refractory hypercalcemia secondary to parathyroid hormone-related protein (PTHrP) secretion. Both the fusion partner, and the presentation of this case of NMC carry particular rarity.
Case Report: A 51-year-old female patient presented to her local Emergency Department with palpitations and was found to have a severely elevated calcium at 4.8 mmol/L (normal range 2.20–2.60 mmol/L). She was admitted and treated aggressively with intravenous fluids, zoledronic acid and denosumab. Her parathyroid hormone (PTH) was suppressed, but her PTHrP was too high to be measured. Further investigation in the form of a computed tomography (CT) chest, abdomen, and pelvis identified a large pulmonary mass and multiple bony metastases. The patient’s calcium level proved resistant to medical treatment, and her consciousness level reduced, leading to admission to Intensive Care for hemofiltration. An endobronchial biopsy and tumor molecular diagnostics identified the presence of a rare BRD3::NUTM1 fusion. Despite correction of her calcium, the patient did not regain full consciousness, and the difficult decision was made to stop active treatment.
Conclusion: This case describes a rare fusion pulmonary NMC presenting with hypercalcaemia and PTHrP secretion. It adds to the literature surrounding this aggressive cancer type, and highlights the need for early tissue diagnosis and immunohistochemistry in atypical and aggressive lung cancers.
Keywords: BRD3, Hypercalcemia, NUTM1, PTHrP
Introduction
We present the case of a 51-year-old female presenting with refractory hypercalcemia secondary to a PTHRrP-secreting lung cancer with a BRD3::NUTM1 fusion. Nuclear protein in testis midline carcinomas, defined by a NUTM1 fusion on immunohistochemistry, are a rare and aggressive cancer type with poor survival outcomes. Predominantly affecting children and young adults [1],[2],[3], around 300 cases have been identified in the literature since 1991, though the true incidence is likely higher than this due to lack of diagnosis (in cases where patients are too unwell at presentation for diagnostic biopsy) and lack of international registration (necessary for identifying patterns or common populations but not carried out in all centers) [4].
Nuclear protein in testis midline carcinomas are driven by gene rearrangement, with fusion of the NUT gene on chromosome 15 with other genes, most commonly BRD4 on chromosome 19 [5]. Other fusions do occur (Table 1) and on very rare occasions this can include a BRD3::NUTM1 fusion [5], as in this case. Often referred to as NUT midline carcinomas due to their predilection for occurring in the midline, these solid tumors are found in the lung, central nervous system, head, neck, and kidneys [3]. The literature reports a median overall survival rate between 4.1 and 7.5 months and pulmonary tumors, regardless of mutation, have the worst outcomes [6].
From a cytopathological perspective, NMCs are poorly differentiated and can have non-specific appearances, which appear to mimic other solid cancers. This can lead to them being initially wrongly diagnosed, particularly as a squamous cell carcinoma or a neuroendocrine tumor, before immunohistochemistry is used to rule out these more common differentials. Molecular diagnostics then identifies the characteristic NUT rearrangement [7].
These cancers are underdiagnosed with limited treatment options and a median survival between two and seven months. This report documents the first presentation—to our knowledge—of a NUT pulmonary carcinoma with PTHrP-secretion-driven hypercalcemia in the literature. This case of NUT carcinoma carries exceptional rarity due to the presence of the NUTM1::BRD3 fusion, as opposed to more common fusions, in addition to it being the first reported case of NMC presenting with hypercalcemia secondary to PTHrP-secretion. The rarity of this case adds to the literature seeking to increase understanding of NUTM1 fusions. It encourages physicians to consider NMC in atypical cases, and highlights the importance of ongoing research to identify potential treatments.

Case Report
A 51-year-old female patient presented to her local Emergency Department with palpitations. She had a past medical history of depression, osteoarthritis, and fibroids and regular medications of citalopram 20 mg once daily. She was a marketing director and a never-smoker. She had additional symptoms of cough, hemoptysis, weight loss, fatigue, anorexia and nausea, which had been present for a number of weeks before her presentation.
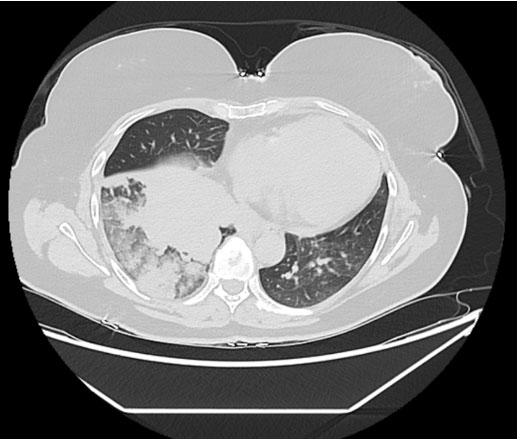
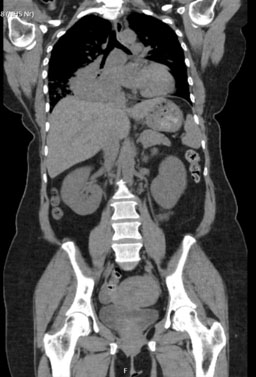
On admission, her laboratory results showed: elevated calcium (4.8 mmol/L), acute kidney injury (urea 17.3 and creatinine 176), a raised alkaline phosphatase (ALP) (168) with normal vitamin D (56) and PTH (1 pmol/L—appropriately suppressed). An electrocardiogram (ECG) showed normal sinus rhythm with left axis deviation, and an admission chest X-ray showed a large area of opacification in the right lung base. She was treated with intravenous fluids and received a first dose of zoledronic acid (4 mg intravenous). She underwent a computed tomography scan of her chest, abdomen and pelvis which showed a large right-sided pulmonary mass with maximum dimension of 8 cm, significant mediastinal lymphadenopathy and narrowing of the right main and lower lobe bronchus, and multiple bony metastases (Figure 1 and Figure 2). There was sparing of the left lung.
Her calcium normalized with 10 days of rehydration, and she was discharged for ongoing investigation under the lung cancer diagnostic team, with an outpatient positron-emission topography-computed tomography (PET-CT), magnetic resonance imaging (MRI) head and endobronchial ultrasound (EBUS). She was readmitted five days later as repeat bloods showed a deterioration in her calcium to 3.96 mmol/L.
Her PET-CT identified that the pulmonary mass was metabolically active and concerning for a primary bronchogenic malignancy, and identified extraosseous soft tissue encroachment of an L2 vertebral metastasis, concerning for cord compression. A follow-up whole spine MRI found multilevel metastatic vertebral marrow infiltration but no evidence of metastatic cord or cauda equina compression. An endobronchial biopsy was performed via bronchoscopy and tissue sent for diagnostics. Her MRI head with contrast found no evidence of metastatic disease.
She received two doses of denosumab 60 mg (five days apart) and started on calcitonin (100 micrograms three times daily, orally). Her PTHrP was too high to be measured, P1NP was 169.6 µg/L (range 51–59) and CTX 4.43 µg/L (range 0.05–0.45). Despite this, her calcium remained above 3 mmol/L and she became progressively confused with fluctuating consciousness. She was admitted to intensive care for hemofiltration while awaiting diagnostic results, which brought her calcium to below 3 mmol/L, without any clinical improvement.
Tumor molecular diagnostics revealed: BRD3 (NM_007371.3) exon 10:: NUTM1 (NM_001284293.1) exon 2. A CT head with contrast showed no other reason for her reduced consciousness, and following discussions with endocrinology and oncology, the difficult decision was made to palliate her. She died three days later surrounded by her family, 52 days from her initial presentation.
Discussion
NUTM1 mutations
Nuclear protein in testis carcinomas are a rare and aggressive cancer type which occur in the midline and are characterized by the fusion of the NUT gene to anther gene as a consequence of gene re-arrangement. In addition to being underdiagnosed, NMCs are often identified late, with evidence showing that early diagnosis and treatment improves survival outcomes [8]. Early diagnosis also allows for enrolment into clinical trials, which have the highest chance of a good survival outcome as compared to conventional therapy. One meta-analysis (54 patients) investigating treatments for NMC found that no conventional chemotherapy improved overall survival or progression free survival; but surgical resection and radiotherapy for tumor reduction were independent predictors of survival, and slowed tumor progression [8]. Due to their central location and aggressive local invasion, surgery or resection is rarely an option for pulmonary NMC, which partly explains the poor survival rates associated with them.
As in this case, pulmonary NMC have been found to present with cough and hemoptysis. A case series investigating eight pulmonary NMC [9] found that at presentation most patients had: little or no smoking history, aggressive local spread, sparing of the contralateral lung, lytic bone lesions, and absence of brain metastasis (unusual for aggressive lung cancers). All of these features were present in the patient in this case. In our search of the literature, we did not find another case of pulmonary NMC presenting with the severe and refractory hypercalcemia seen here.
PTHrP
Malignant hypercalcemia (HCM) is relatively common and is seen mainly in breast, lung, and bone cancer [10]. It is most commonly humoral (driven by tumor secretion of PTHrP) or due to osteolytic metastases. There is a poor prognosis associated with HCM, although this has improved with the introduction of new anticancer treatments [11]. Management of humoral HCM requires aggressive treatment with fluid replacement, bisphosphonates, denosumab, and (in severe cases) calcitonin. But tumor reduction to stop PTHrP secretion is the mainstay of treatment, and without this medical management will always be limited. The severe and refractory hypercalcemia in this case meant that the patient’s prognosis was poor pre-molecular testing; and, once diagnosed, the lack of tumor reducing treatments meant that the survival outcome was poor at best.
Key learning points
- Despite significant advances in anti-cancer treatments over the last 10 years, there remain cancers for which we have few treatment options, and prognosis in these cases can be poor.
- Malignant hypercalcemia at presentation remains a poor prognostic factor, even where cancer specific treatment is available.
- For rare cancer types like NMC, early molecular diagnosis is vital in allowing treatment options to be explored through clinical trials and tumor reducing surgery, and registration of these cancers is essential for future research.
- Clinicians should be aware of rare cancer types and identify patients in whom these could be present, to attempt to expedite diagnostic testing and identification.
- Patients with pulmonary NMC may be diagnosed with cancer and die shortly after. This can be difficult for families to come to terms with. It is important that oncologists and the wider multidisciplinary team are aware of this, and can proactively find time to support families and answer the questions that they have.
Conclusion
Hypercalcemia and PTHrP secretion have not previously been associated with a pulmonary NMC. This cancer type and the BRD3::NUTM1 fusion are incredibly rare, and the addition of a PTHrP driven hypercalcemia makes this case rarer still. This case adds new information to the literature surrounding this aggressive cancer type. It highlights the importance of early tissue diagnosis and immunohistochemistry in atypical lung cancers, to identify rare carcinomas and allow early treatment through clinical trials. Finally, as the definitive management of malignant hypercalcemia is tumor reduction, this case emphasizes the urgent need for further research to identify treatment options for NUT carcinomas.
REFERENCES
1.
Jha P, Trivedi V, Menon N, Shah M, George IA, Mishra R, et al. NUT-midline carcinoma of the lung with rare BRD3-NUTM1 fusion. Cancer Research, Statistics, and Treatment 2024;7(1):110–6. [CrossRef]

2.
French C. NUT midline carcinoma. Nat Rev Cancer 2014;14(3):149–50. [CrossRef]
[Pubmed]
3.
Sanchez Becerra MV, Knetki-Wroblewska M, O’Reilly S, Bover Larroya M, Benitez Montañez JC, Martin Martorell P. 147O Scope of NUT carcinomas (NC): An international multicentric study. ESMO Open 2024;9(Suppl 2):102542. [CrossRef]
4.
Lauer UM, Hinterleitner M, Horger M, Ohnesorge PV, Zender L. NUT carcinoma—An underdiagnosed malignancy. Front Oncol 2022;12:914031. [CrossRef]
[Pubmed]
5.
Luo W, Stevens TM, Stafford P, Miettinen M, Gatalica Z, Vranic S. NUTM1-rearranged neoplasms—A heterogeneous group of primitive tumors with expanding spectrum of histology and molecular alterations—An updated review. Curr Oncol 2021;28(6):4485–503. [CrossRef]
[Pubmed]
6.
Kloker LD, Sidiras M, Flaadt T, Brecht IB, Deinzer CKW, Groß T, et al. Clinical management of NUT carcinoma (NC) in Germany: Analysis of survival, therapy response, tumor markers and tumor genome sequencing in 35 adult patients. Lung Cancer 2024;189:107496. [CrossRef]
[Pubmed]
7.
Bishop JA, French CA, Ali SZ. Cytopathologic features of NUT midline carcinoma: A series of 26 specimens from 13 patients. Cancer Cytopathol 2016;124(12):901–8. [CrossRef]
[Pubmed]
8.
Bauer DE, Mitchell CM, Strait KM, Lathan CS, Stelow EB, Lüer SC, et al. Clinicopathologic features and long-term outcomes of NUT midline carcinoma. Clin Cancer Res 2012;18(20):5773–9. [CrossRef]
[Pubmed]
9.
Sholl LM, Nishino M, Pokharel S, Mino-Kenudson M, French CA, Janne PA, et al. Primary pulmonary NUT midline carcinoma: Clinical, radiographic, and pathologic characterizations. J Thorac Oncol 2015;10(6):951–9. [CrossRef]
[Pubmed]
10.
Shieh A, Martinez D. Hypercalcaemia of malignancy. BMJ Best Practice. 18 July 2023. [Available at: https://bestpractice.bmj.com/topics/en-gb/1204]
11.
Mc Donald D, Drake MT, Crowley RK. Treatment of hypercalcaemia of malignancy in adults. Clin Med (Lond) 2023;23(5):503–7. [CrossRef]
[Pubmed]
12.
Stevens TM, Morlote D, Xiu J, Swensen J, Brandwein-Weber M, Miettinen MM, et al. NUTM1-rearranged neoplasia: A multi-institution experience yields novel fusion partners and expands the histologic spectrum. Mod Pathol 2019;32(6):764–73. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We would like to thank the next of kin of this patient, who gave their informed consent for the use and disclosure of her health information here.
Artificial intelligence (AI) use in the article: none.
Rosa Evans - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Keziah Abbotts - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Emma Mclean - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Thomas Simpson - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Alexandros Georgiou - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Spyridon Gennatas - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Rosa Evans et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}