 |
Case Report
Desmoplastic small round cell tumor of abdomen: Case report of a very rare sarcoma with diagnostic challenge
1 Consultant Medical Oncology, Adult Medical Oncology Department, King Fahad Hospital, Medina, Saudi Arabia
2 Assistant Professor of Molecular Pathology, Clinical Laboratory Science Department, Faculty of Applied Medical Science, Taibah University, Medina, Saudi Arabia
3 Assistant Professor, Faculty of Medicine, Taibah University, Medina, Saudi Arabia
4 Consultant Medical Oncology, Adult Oncology Department, King Salman Specialist Hospital, Hail, Saudi Arabia
Address correspondence to:
Samir Alfotih
King Fahad Hospital, Medina,
Saudi Arabia
Message to Corresponding Author
Article ID: 100084Z10SA2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Alfotih S, Zahid H, Mulla N, Wazir KB. Desmoplastic small round cell tumor of abdomen: Case report of a very rare sarcoma with diagnostic challenge. J Case Rep Images Oncology 2021;7:100084Z10SA2021.ABSTRACT
Introduction: A desmoplastic small round blue cell tumor (DSRCT) is a very rare soft tissue sarcoma. The first case was reported in 1989 by Gerald and Rosai. Diagnosis can be challenging, and a differential diagnosis should be considered when a young patient presents with wide-spread abdominal disease without definitive organ involvement as shown in imaging studies. A typical radiological finding in DSRCT is a dominant solid mass in a retrovesical or rectouterine pouch with widespread peritoneal nodules.
Case Report: In this case report, we present a case of a very rare sarcoma in a young Saudi male patient who presented with abdominal distension and widespread intra-abdominal disease with liver metastases. The dominant mass had a cystic component and was not in a typical site.
Conclusion: Diagnosis of such sarcoma is challenging and it needs the correlation of clinical, radiological, morphological, immunohistochemical, and even genetic data.
Keywords: Desmoplastic small round cell tumor, Diagnosis, Radiological finding
Introduction
A desmoplastic small round blue cell tumor (DSRCT) is a very rare soft tissue sarcoma tumor, usually arises from intra-abdominal mesenchymal tissues and it has very aggressive clinical behavior. Since the first case of DSRCT reported in 1989 by Gerald and Rosai [1], approximately 500 cases have been described in the literatures [2],[3].
Desmoplastic small round blue cell tumors mainly present in children and young adults. The main symptoms are related to widespread intra-abdominal disease. Almost all patients have peritoneal metastases at presentation, and approximately half of the presenting patients have extra-peritoneal metastases (EPM) [3]. Diagnosis depends on correlation of clinical presentation with positivity of different immunohistochemical (IHC) markers (epithelial, mesenchymal, neural, and muscle), but the most characteristic marker is the presence of the EWS-WT1 protein [4],[5]. The prognosis of this type of sarcoma is dismal. Despite the use of different treatment modalities, including surgery, radiation, and chemotherapy, the 5-year survival is still around 15% [6].
We present a case of a very rare soft tissue sarcoma in a young Saudi male patient who was diagnosed from a biopsy obtained from a metastatic site (liver) rather than the primary site.
Case Report
Patient information
A 32-year-old male patient without known medical disease presented to our hospital with rapidly progressive abdominal distension of two months duration associated with mild dull aching abdominal pain and weight loss of 1 kilogram.
Clinical findings
His clinical examination was remarkable for tense ascites, and an ill-defined abdominal mass was found in the umbilical area.
Diagnostic assessment
Initial workup showed mild thrombocytosis but blood counts, liver, and renal function were normal.
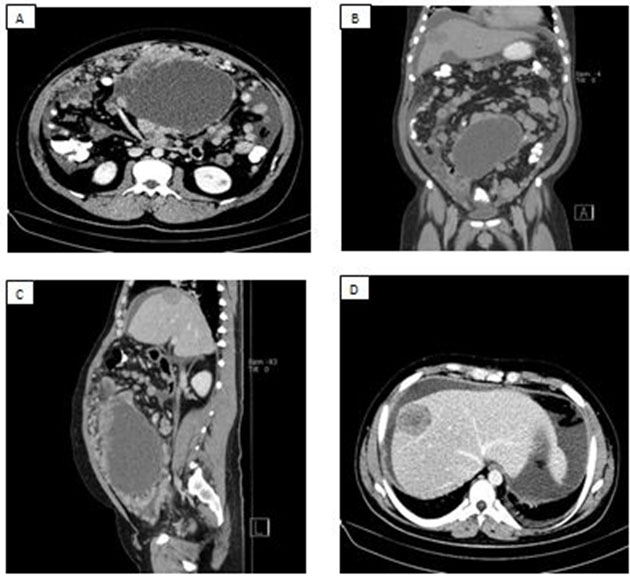
His initial workup was based on abdominal ultrasound and showed ascites and multiple liver masses, so the patient had an abdominal computed tomography (CT) scan with contrast, which revealed a large, predominantly cystic mass measuring 16.5 × 15 × 12.5 cm arising from the mesentery that had displaced the small bowel loops. In addition, the CT showed ascites, multiple peritoneal nodules, and cystic liver metastases (Figure 1).
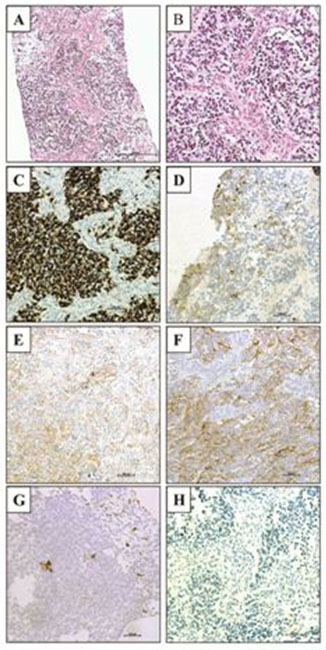
Because of the tense ascites, 4 L was aspirated and was sent for cytological examination, which showed the presence of atypical cells. The patient underwent ultrasound (US)-guided biopsy from the liver mass. A sheet of round small cells was observed. Based on the liver biopsy, our pathologist recognized a desmoplastic stroma between the cells.
IHC method
Immunohistochemistry was performed at King Fahad General Hospital histopathology laboratory using the Ventana Discovery XT. Briefly, 4 μm paraffin sections were deparaffinized. Tris-EDTA buffer pH 7.8 at 95 °C for 44 min was used for antigen retrieval. Primary antibodies were incubated for 1 hour whereas horseradish peroxidase (HRP)-conjugated secondary antibodies were incubated for 16 minutes. DAB was applied for 8 minutes followed by 8 minutes of counterstain with hematoxylin. Slides were dehydrated and coverslipped.
The malignant cells showed strong positive desmin and were weakly positive for pan-cytokeratin (CK-pan), cluster of differentiation (CD)99, and CD56 but negative for CD45, low-molecular weight cytokeratin (LMWCk), S100, and neuron-specific enolase (NSE) (Figure 2). A diagnosis of an abdominal desmoplastic small round blue cell tumor (DSRCT) with liver metastases was made.
Therapeutic intervention, follow-up, and outcomes
Since this tumor is very rare, we referred the patient to a hospital specialized in treating such rare tumors in the kingdom. Pathology was reviewed in the accepted hospital, and it is concurred with our diagnosis.
Discussion
Desmoplastic small round blue cell tumor is a very rare soft sarcoma and presents a highly aggressive clinical course that affects mainly young males of Caucasian ethnicity [7]. It was first described by Gerald and Rosai in 1989. They described a tumor with characteristic features containing small blue round cells that are surrounded by desmoplastic stroma. Those cells can express epithelial, neuronal, and mesenchymal markers. Up to now, approximately 500 cases of DSRCT have been reported in the literature. To the best of our knowledge, only five DSCRT cases have been reported in Saudi Arabia (two intra-abdominal, one ovarian, one stomach, and one pancreatic).
Desmoplastic small round blue cell tumors are typically seen in the abdominal or pelvic cavity in 90% of patients, but a wide spectrum of rare sites including testis, pleura, stomach, pancreases, kidney, sinus, and brain have been reported [7],[8].
Desmoplastic small round blue cell tumor is a disease of adolescent males with a male to female ratio of 4:1. The usual presentation of most of cases is in the second or third decade of life [9]. Since the most common site of a DSRCT is intra-abdominal, most patients present with gastrointestinal symptoms. Unfortunately, those symptoms occur when the tumor is at an advanced stage as seen in our case. At this point, approximately half of patients present with metastases, and the most common metastases are liver, lung, and lymph nodes [2],[8].
Imaging studies in DSRCT do not show specific findings, but these findings suggest this disease when a young patient presents with an abdominal or pelvic mass with extensive peritoneal disease and ascites without definitive organ involvement [7]. The dominant mass is lobulated, solid, and shows a retrovesical or rectouterine location with an average size of 12 mm in more than 50% of patients [10]. Our patient presented with a huge abdominal mass (16 cm) with peritoneal nodules, ascites, and liver metastases. The mass in our patient has a cystic component, and its location is not a typical radiological feature. In a small retrospective study, it was found that fluorodeoxyglucose-positron emission/computed tomography (FDG-PET/CT) showed superiority to conventional imaging for detecting disease burden, and in another study, it was found that PET/CT has advantages over conventional imaging for detecting isolated relapses [10].
Even after a biopsy of a DSRCT tumor, the diagnosis may still be challenging because, microscopically, the tumor appears as round blue cells with the possibility for many differential diagnoses, for example, Ewing’s sarcoma. However, the presence of extensive collagenous stroma points to the correct diagnosis. Furthermore, by using IHC, the tumor was shown to co-express many marker (epithelial, mesenchymal, neural, and muscle). In our case, the biopsy was taken from the metastatic site (liver). The most important confirmatory test, which is found in more than 90% of patients, was the presence of the translocation t(11;22) (p13;q12) and detection of EWS-WT1 gene by reverse transcriptase polymerase chain reaction [4],[5].
Unfortunately, no standard treatment for DSRCT is available to date because of the very rare nature of the tumor, which makes it extremely difficult to conduct clinical trials. Furthermore, no validated staging system exists for comparing different treatment approaches of this tumor. The recommendation of multimodal treatment consisting of surgery, radiation, and chemotherapy in suitable patients is based on retrospective studies. Lal et al. reported that the 3-year survival for patients who were treated with induction chemotherapy (P6), debulking surgery, and radiotherapy is 55% compared with only 27% in those who are not treated with this method. Despite this difference and even after using the aggressive approach for treating these tumors, the prognosis is dismal and the 5-year survival is only 15%. In recent retrospective study, the 5-year survival reported is only 25% by using multidisciplinary treatment [9].
Conclusion
We present a case of a DSCRT, a rare soft tissue sarcoma, which is a highly aggressive tumor. Its diagnosis may be challenging and needs the correlation of clinical, radiological, morphological, immunohistochemical, and even genetic data to reach a diagnosis, especially in atypical presentations.
REFERENCES
1.
Gerald WL, Rosai J. Case 2. Desmoplastic small cell tumor with divergent differentiation. Pediatr Pathol 1989;9(2):177–83. [CrossRef]
[Pubmed]

2.
Dufresne A, Cassier P, Couraud L, Marec-Bérard P, Meeus P, Alberti L, Blay YJ. Desmoplastic small round cell tumor: Current management and recent findings. Sarcoma 2012;2012:714986. [CrossRef]
[Pubmed]
3.
Honoré C, Amroun K, Vilcot L, et al. Abdominal desmoplastic small round cell tumor: Multimodal treatment combining chemotherapy, surgery, and radiotherapy is the best option. Ann Surg Oncol 2015;22(4):1073–9. [CrossRef]
[Pubmed]
4.
Doyle LA. Sarcoma classification: An update based on the 2013 World Health Organization classification of tumors of soft tissue and bone. Cancer 2014;120(12):1763–74. [CrossRef]
[Pubmed]
5.
Mora J, Modak S, Cheung NK, et al. Desmoplastic small round cell tumor 20 years after its discovery. Future Oncol 2015;11(7):1071–81. [CrossRef]
[Pubmed]
6.
Bent MA, Padilla BE, Goldsby RE, DuBois SG. Clinical characteristics and outcomes of pediatric patients with desmoplastic small round cell tumor. Rare Tumors 2016;8(1):6145. [CrossRef]
[Pubmed]
7.
Lae ME, Roche PC, Jin L, Lloyd RV, Nascimento AG. Desmoplastic small round cell tumor: A clinicopathologic, immunohistochemical, and molecular study of 32 tumors. Am J Surg Pathol 2002;26(7):823–35. [CrossRef]
[Pubmed]
8.
Lettieri C, Garcia-Filion P, Hingorani P. Incidence and outcomes of desmoplastic small round cell tumor: Results from the surveillance, epidemiology, and end results database. J Cancer Epidemiol 2014;2014:680126. [CrossRef]
[Pubmed]
9.
Subbiah V, Lamhamedi-Cherradi S, Cuglievan B, et al. Multimodality treatment of desmoplastic small round cell tumor: Chemotherapy and complete cytoreductive surgery improve patient survival. Clin Cancer Res 2018;24(19):4865–73. [CrossRef]
[Pubmed]
10.
Arora VC, Price AP, Fleming S, et al. Characteristic imaging features of desmoplastic small round cell tumour. Pediatr Radiol 2013;43(1):93–102. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Samir Alfotih - Acquisition of data, Analysis of data, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Heba Zahid - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nasser Mulla - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Khaled Ba Wazi - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Samir Alfotih et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}