 |
Case Series
Lumbar hernias: The simplicity of open repair
1 BSc, MD, MS, General Surgical Registrar, Department of General Surgery, Austin Hospital, Heidelberg, Victoria, Australia
2 MBBCh, FCS (SA), FRACS, General Surgeon, Department of General Surgery, Central Gippsland Health, Victoria, Australia
Address correspondence to:
Maryum Qureshi
Austin Hospital, 145 Studley Road, Heidelberg, VIC 3084,
Australia
Message to Corresponding Author
Article ID: 101493Z01MQ2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Qureshi M, Strauss P. Lumbar hernias: The simplicity of open repair. Int J Case Rep Images 2025;16(1):24–28.ABSTRACT
Introduction: Lumbar hernias are an extremely rare condition characterized by a defect in the posterior abdominal wall. Surgical repair is the recommended treatment to prevent strangulation, obstruction, incarceration, or perforation of abdominal contents within the hernia sac.
Case Series: In this case series, we present two patients with a lumbar hernia. A 52-year-old male presented with a traumatic right inferior lumbar hernia containing the base of cecum and appendix, and an 84-year-old female presented with an iatrogenic left inferior lumbar hernia containing descending colon. Both patients underwent a successful open repair of the hernia with insertion of an extraperitoneal polypropylene mesh. Their recovery was uneventful and both patients were discharged on the first postoperative day with no complications on follow up.
Conclusion: Lumbar hernia is a rare clinical entity. An inferior lumbar hernia is more uncommon than a superior lumbar hernia. We present two cases managed with safe, effective and reproducible surgical treatment.
Keywords: Extraperitoneal mesh, Incarceration, Lumbar hernia, Open surgical repair, Strangulation
Introduction
Lumbar hernias are described as a defect that occur in the posterior abdominal wall. The first case of lumbar hernia was published in 1731 by DeGarangeot [1]. They represent 1.5–2% of all abdominal wall hernias [2]. Given the rarity of the condition, lumbar hernias are not commonly seen by surgeons and can be misdiagnosed leading to significant morbidity [3]. A thorough history, clinical examination, and computed tomography (CT) imaging are essential for diagnosis and preoperative planning. Surgical repair with mesh remains the standard of treatment to avoid complications such as strangulation (8% risk), obstruction, incarceration (25–30% risk), or perforation of abdominal contents within the hernia sac [1],[2]. The traditional open surgical approach has been widely reported as a common technique for the repair of lumbar hernias [1],[4],[5],[6],[7]. We report two cases of lumbar hernias managed successfully with open surgical repair.
CASE SERIES
Case 1
A 52-year-old male referred to surgical outpatients by the General Physician (GP) with a potential lipoma, presenting with right flank pain and a lump in the right lower lumbar region. His significant comorbidities were obesity, rheumatoid arthritis treated with methotrexate and prednisolone, gastroesophageal reflux managed with esomeprazole, well established chronic obstructive pulmonary disease (COPD) controlled with tiotropium and ventolin and chronic pain managed with buprenorphine. The patient had no abdominal surgical history. On further history, the patient was found to be involved in a significant motor vehicle accident many years ago.
On examination, there was a tender, right lumbar mass superior to the iliac spine, likely a lumbar hernia secondary to traumatic injury with rupture of muscle and a subsequent hematoma. Computed tomography abdomen and pelvis demonstrated a right posterolateral abdominal wall hernia measuring approximately 55 mm anteroposteriorly and 48 mm craniocaudally. There was herniation of omental fat and appendix through this defect (Figure 1A and Figure 1B). On further review, the patient was consented and booked for an open repair of the hernia and placement of a sublay mesh due to underlying respiratory illness and immunocompromised state.
The hernia site was marked preoperatively with the patient standing (Figure 2). General anesthetic was administered. The patient was placed in the left lateral position and the bed broken to widen the 12th rib and iliac crest distance. An incision was made parallel and superior the right iliac crest. With retraction and dissection, the defect was located. The edges of the hernial defect were defined with retraction and dissection in a circumferential fashion. The pre-peritoneal space was entered, and a large pocket created with a combination of blunt and sharp dissection. The peritoneum and pre-peritoneum were separated widely across the iliac blade and muscles anterior and posterior (Figure 3). A bard Ventrio hernia mesh (11×14 cm) was placed in the pre-peritoneal space with at least 5 cm overlap (Figure 4). The mesh was secured inferiorly with endo tackers to the iliac blade. The wound was closed in layers including the defect. No drain was placed.
Case 2
An 84-year-old female was similarly referred to outpatient surgical clinic for opinion and management of a newly diagnosed loin lump with a differential diagnosis of a lipoma. The past medical history was significant of well controlled hypertension, hyperlipidemia and COPD. The patient was a non-smoker.
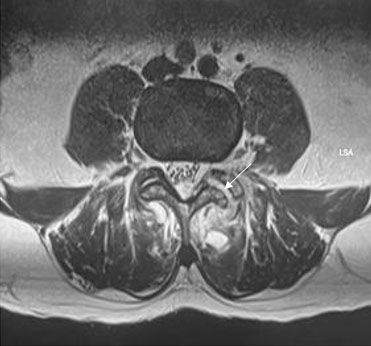
On clinical examination, the patient had a completely reducible left lumbar hernia. The diagnosis was subsequently confirmed on CT abdomen, pelvis demonstrating a left sided inferior lumbar hernia measuring 41 mm × 33 mm containing unobstructed descending colon and omentum (Figure 5A and Figure 5B). The patient was therefore booked for an urgent repair due to high risk of strangulation and subsequent morbidity.
The procedure was performed in identical fashion as the previous patient; however, a smaller-sized mesh was used (Figure 6, Figure 7, Figure 8). Both patients had an uneventful recovery and were discharged the following day. On subsequent follow-up, there were no surgical issues.








Discussion
Lumbar hernias are defined as a rare defect in the posterolateral abdominal wall. They are characterized by the protrusion of intra-abdominal or extraperitoneal contents through the defect. They account for 2% of all hernias and are more common in males and on the left side [2],[8],[9]. A lumbar hernia can present as an asymptomatic bulge in the lower back or with symptoms of flank or back pain which may be exacerbated by straining, heavy lifting, coughing, or sneezing [2]. Patients may suffer from altered bowel habits or constipation if the hernia contains bowel [10]. Lumbar hernias can be subdivided into categories based on etiology and anatomical location. They are either congenital (20%) or acquired (80%) [3],[8]. Acquired lumbar hernias can be primary or secondary [1],[3],[8],[11]. Primary acquired lumbar hernias can occur in patients with obesity, poor nutrition, connective tissue disease, muscle weakness, or conditions that increase intra-abdominal pressure [4]. Secondary acquired lumbar hernias can occur following surgery in the retroperitoneum or flaps for breast reconstruction, or following trauma, infection, or inflammation [8],[10]. Risk factors include obesity, short stature, or anatomically large triangles [12].
The hernias can be divided into two anatomical locations—superior lumbar triangle (Grynfelt-Lesshaft) and inferior lumbar triangle (Petit). Superior lumbar hernias are more common due to the larger surface area [11].
Anatomical borders of the Grynfelt triangle include the twelfth rib and serratus posterior inferior muscle at its base, external oblique, and latissimus dorsi muscle at its roof, aponeurosis of transversus abdominis as the floor, internal oblique muscle anteriorly, and sacrospinalis muscle posteriorly [10],[13],[14]. Petit triangle is bordered inferiorly by the iliac crest, medially by the lateral edge of latissimus dorsi, laterally by the medial edge of external oblique and posteriorly by the superficial fascia and skin [15].
A thorough history and clinical examination are essential for diagnosis to determine possible etiology and reducibility of the hernia. Given the rarity of the condition, these hernias are commonly misdiagnosed as lipoma, fibroma, hematomas, retroperitoneal tumor, abscess, perirenal abscess or tumor or muscle strain [3],[16]. Imaging with CT or magnetic resonance imaging (MRI) is essential to confirm the diagnosis, identify the anatomical location of the hernia and the contents of the hernia [16]. Imaging is particularly useful for preoperative planning and urgency of surgical intervention.
Surgical repair is the mainstay of treatment for lumbar hernias. Observation can over time lead to widening of the defect and further weakness of the surrounding musculature and tissue which makes the hernia repair more difficult [10]. There is no standard surgical approach for the management of lumbar hernia due to the rarity of the condition. The open surgical approach is well established, safe, and effective [1],[4],[5],[6],[7]. In recent years, there has been an increase in laparoscopic repair of lumbar hernias for smaller defects where abdominal wall reconstruction is not required [16]. Laparoscopic repair allows for better visualization of the hernial defect, nerve pathways, and secure mesh placement [10],[11]. However, it is associated with technical difficulty, increased risk of organ injury, and chronic pain from mesh tacking [11]. Open surgery is recommended for patients with larger defects (traumatic or diffuse), adhesions from previous surgeries or comorbidities preventing prolonged pneumoperitoneum [16]. The traditional open approach allows for parietal reconstruction and repair under controlled tension [6]. Surgical approach for lumbar hernias depends on patient factors, size of the defect, healthcare facilities, and surgical expertise [1]. Recurrence after surgical repair is the main long-term effect. Patients with diffuse hernias or a defect larger than 16 cm have an increased risk of recurrence. Literature reports an overall recurrence rate of 2–3% [1]. A medium to heavy weight polypropylene mesh with a minimum overlap of 6 cm with adequate fixation is recommended to prevent recurrence [6].
Conclusion
Protrusion of intra-abdominal contents through a defect in the muscles of the lumbar region. Early diagnosis and treatment are essential in decreasing overall morbidity and mortality associated with delayed diagnosis or complications such as strangulation with gangrenous bowel or obstruction. Although rare, lumbar hernias should be considered in patients presenting with a bulge or lump in the flank or in patients who have intestinal obstruction, especially in elderly patients. Mortality is associated with delayed presentation and diagnosis.
REFERENCES
1.
Shen C, Zhang G, Zhang S, et al. Clinical, surgical characteristics and long-term outcomes of lumbar hernia. BMC Surg 2021;21(1):332. [CrossRef]
[Pubmed]

2.
Shankar A, Selvaraj K, Kumar P, Pattabi S. Sandwiching a lumbar hernia: A case report. Cureus 2024;16(10):e71590. [CrossRef]
[Pubmed]
3.
Ahmed ST, Ranjan R, Saha SB, Singh B. Lumbar hernia: A diagnostic dilemma. BMJ Case Rep 2014;2014:bcr2013202085. [CrossRef]
[Pubmed]
4.
Cavallaro G, Sadighi A, Paparelli C, et al. Anatomical and surgical considerations on lumbar hernias. Am Surg 2009;75(12):1238–41.
[Pubmed]
5.
Cavallaro G, Sadighi A, Miceli M, Burza A, Carbone G, Cavallaro A. Primary lumbar hernia repair: The open approach. Eur Surg Res 2007;39(2):88–92. [CrossRef]
[Pubmed]
6.
Moreno-Egea A, Baena EG, Calle MC, Martínez JAT, Albasini JLA. Controversies in the current management of lumbar hernias. Arch Surg 2007;142(1):82–8. [CrossRef]
[Pubmed]
7.
Moreno-Egea A, Alcaraz AC, Cuervo MC. Surgical options in lumbar hernia: Laparoscopic versus open repair. A long-term prospective study. Surg Innov 2013;20(4):331–44. [CrossRef]
[Pubmed]
8.
Rafols M, Bergholz D, Andreoni A, Knickerbocker C, Davies J, Grossman RA. Bilateral lumbar hernias following spine surgery: A case report and laparoscopic transabdominal repair. Case Rep Surg 2020;2020:8859106. [CrossRef]
[Pubmed]
9.
Fokou M, Fotso P, Ngowe Ngowe M, Essomba A, Sosso M. Strangulated or incarcerated spontaneous lumbar hernia as exceptional cause of intestinal obstruction: Case report and review of the literature. World J Emerg Surg 2014;9:44. [CrossRef]
[Pubmed]
10.
Kawakami K, Moriwaki Y, Otani J. A case of idiopathic superior lumbar hernia repaired using a transabdominal laparoscopic approach. J Surg Case Rep 2024;2024(10):rjae608. [CrossRef]
[Pubmed]
11.
Lin R, Teng T, Lin X, et al. Sublay repair for primary superior lumbar hernia with the Kugel patch. ANZ J Surg 2020;90(5):776–80. [CrossRef]
[Pubmed]
12.
Khoo JF, Chua TC. Laparoscopic transabdominal preperitoneal repair of lumbar hernia. ANZ J Surg 2022;92(10):2688–9. [CrossRef]
[Pubmed]
13.
Loukas M, El-Zammar D, Shoja MM, et al. The clinical anatomy of the triangle of Grynfeltt. Hernia 2008;12(3):227–31. [CrossRef]
[Pubmed]
14.
Tsouknidas I, Tasis N, Antonopoulou MI, Acheimastos V, Manatakis DK. Traumatic lumbar hernia: A systematic review of the literature. Chin J Traumatol 2024;27(1):53–7. [CrossRef]
[Pubmed]
15.
Loukas M, Tubbs RS, El-Sedfy A, et al. The clinical anatomy of the triangle of Petit. Hernia 2007;11(5):441–4. [CrossRef]
[Pubmed]
16.
Heemskerk J, Leijtens JWA, van Steensel S. Primary lumbar hernia, review and proposals for a standardized treatment. J Abdom Wall Surg 2023;2:11754. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Maryum Qureshi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Paul Strauss - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Maryum Qureshi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



/2025/images/figure1.1740845126.jpg){kind=link}
/2025/images/figure1.1740845126.jpg){kind=link}
/2025/images/figure1.1740845126.jpg){kind=link}
/2025/images/figure1.1740845126.jpg){kind=link}
/2025/images/figure1.1740845126.jpg){kind=link}
/2025/images/figure1.1740845126.jpg&title=Article%20Image){kind=link}
/2025/images/figure1.1740845126.jpg){kind=link}
/2025/images/figure2.1740845126.jpg){kind=link}
/2025/images/figure2.1740845126.jpg){kind=link}
/2025/images/figure2.1740845126.jpg){kind=link}
/2025/images/figure2.1740845126.jpg){kind=link}
/2025/images/figure2.1740845126.jpg){kind=link}
/2025/images/figure2.1740845126.jpg&title=Article%20Image){kind=link}
/2025/images/figure2.1740845126.jpg){kind=link}
/2025/images/figure3.1740149511.jpg){kind=link}
/2025/images/figure3.1740149511.jpg){kind=link}
/2025/images/figure3.1740149511.jpg){kind=link}
/2025/images/figure3.1740149511.jpg){kind=link}
/2025/images/figure3.1740149511.jpg){kind=link}
/2025/images/figure3.1740149511.jpg&title=Article%20Image){kind=link}
/2025/images/figure3.1740149511.jpg){kind=link}
/2025/images/figure4.1740149511.jpg){kind=link}
/2025/images/figure4.1740149511.jpg){kind=link}
/2025/images/figure4.1740149511.jpg){kind=link}
/2025/images/figure4.1740149511.jpg){kind=link}
/2025/images/figure4.1740149511.jpg){kind=link}
/2025/images/figure4.1740149511.jpg&title=Article%20Image){kind=link}
/2025/images/figure4.1740149511.jpg){kind=link}
/2025/images/figure5.1740149511.jpg){kind=link}
/2025/images/figure5.1740149511.jpg){kind=link}
/2025/images/figure5.1740149511.jpg){kind=link}
/2025/images/figure5.1740149511.jpg){kind=link}
/2025/images/figure5.1740149511.jpg){kind=link}
/2025/images/figure5.1740149511.jpg&title=Article%20Image){kind=link}
/2025/images/figure5.1740149511.jpg){kind=link}
/2025/images/figure6.1740149511.jpg){kind=link}
/2025/images/figure6.1740149511.jpg){kind=link}
/2025/images/figure6.1740149511.jpg){kind=link}
/2025/images/figure6.1740149511.jpg){kind=link}
/2025/images/figure6.1740149511.jpg){kind=link}
/2025/images/figure6.1740149511.jpg&title=Article%20Image){kind=link}
/2025/images/figure6.1740149511.jpg){kind=link}
/2025/images/figure7.jpg){kind=link}
/2025/images/figure7.jpg){kind=link}
/2025/images/figure7.jpg){kind=link}
/2025/images/figure7.jpg){kind=link}
/2025/images/figure7.jpg){kind=link}
/2025/images/figure7.jpg&title=Article%20Image){kind=link}
/2025/images/figure7.jpg){kind=link}
/2025/images/figure8.jpg){kind=link}
/2025/images/figure8.jpg){kind=link}
/2025/images/figure8.jpg){kind=link}
/2025/images/figure8.jpg){kind=link}
/2025/images/figure8.jpg){kind=link}
/2025/images/figure8.jpg&title=Article%20Image){kind=link}
/2025/images/figure8.jpg){kind=link}