 |
Case Report
Case of isolated extranodal relapse of diffuse large B-cell lymphoma in the thyroid gland after years of complete remission: A rare presentation
1 Faculty of Medicine and Medical Sciences, University of Balamand, Beirut, Lebanon
2 MD, Faculty of Medicine, Lebanese University, Beirut, Lebanon
Address correspondence to:
Michael Achram
Beirut,
Lebanon
Message to Corresponding Author
Article ID: 100152Z10MA2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Achram M, Yazbek J. Case of isolated extranodal relapse of diffuse large B-cell lymphoma in the thyroid gland after years of complete remission: A rare presentation. J Case Rep Images Oncology 2026;12(1):1–4.ABSTRACT
Introduction: Extranodal recurrence of lymphoma is a phenomenon occurring most commonly within the gastrointestinal (GI) tract, central nervous system (CNS), and skin. Isolated involvement of the thyroid gland is rare and can be mistaken for other conditions such as an inflammatory process without the proper clinical setting.
Case Report: A 64-year-old female patient with a history of lymphoma which was in complete remission for more than a decade presented with a palpable cervical mass. A computed tomography (CT) scan showed a diffusely enlarged thyroid gland without the presence of pathological lymph nodes throughout the body. During the following weeks, the thyroid gland underwent a rapid increase in size causing severe narrowing of the airways which was confirmed by pathology to be due to diffuse large B-cell lymphoma recurrence within the thyroid gland.
Conclusion: A thorough understanding of the patient’s clinical history is crucial for accurate diagnosis, even in rare conditions, and helps prevent delayed initiation of appropriate management.
Keywords: Diffuse large B-cell lymphoma, DLBCL, Extranodal lymphoma, Isolated recurrence, Thyroid lymphoma
Introduction
Lymphoma is a type of cancer that develops from lymphoid cells, which are part of the immune system, and can originate at various stages of their development. The majority, approximately 90%, are derived from B cells [1]. Diffuse large B-cell lymphoma is the most common type of the non-Hodgkin’s lymphoma representing 30% to 40% of all cases. They are more prevalent in the elderly population (median age in the seventh decade of life) with a slight male predominance, and they usually present clinically as a rapidly growing tumoral mass in nodal and/or extranodal sites and B symptoms [1],[2]. Primary extranodal lymphomas are malignancies arising from sites excluding the lymph nodes, spleen, or bone marrow with involvement of its contiguous lymph node group [3]. Approximately one-third of non-Hodgkin’s lymphomas are extranodal with diffuse large B-cell lymphoma being the most encountered type. The most common primary extra nodal site is the gastrointestinal (GI) tract, including the stomach and small intestines, followed by the skin, central nervous system (CNS), and Waldeyer’s ring [4]. Important risk factors for primary extranodal lymphomas include individuals with autoimmune diseases and those that are severely immunocompromised [3].
Case Report
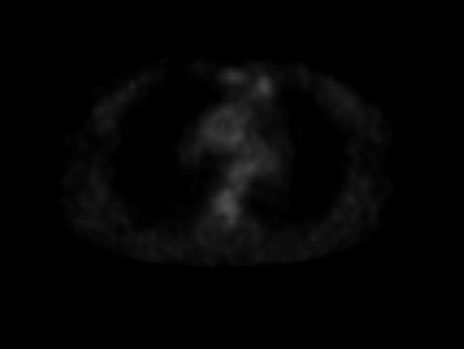
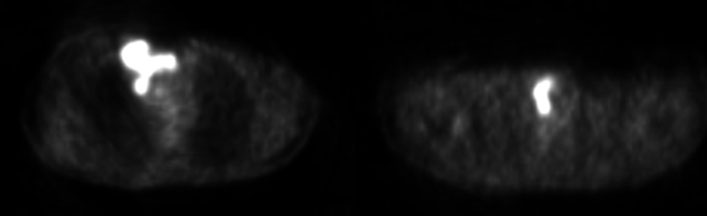
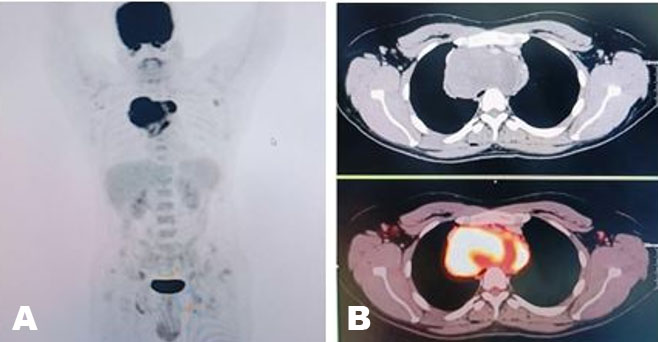
We present the case of a 64-year-old female patient with a history of lymphoma initially presenting to our institution in 2008 when she underwent a total body positron emission tomography-computed tomography (PET-CT) revealing a mildly avid left parasternal mass (Figure 1). A repeat examination three years later revealed progression of disease with the interval appearance of multiple hypermetabolic foci in the right lung and mediastinal regions, including the right parasternal space, right retro-pectoral space and left thyroidal region (Figure 2). After treatment with chemotherapy three months later, a PET-CT scan showed resolution of the previously mentioned hypermetabolic foci and the patient remained in complete remission.
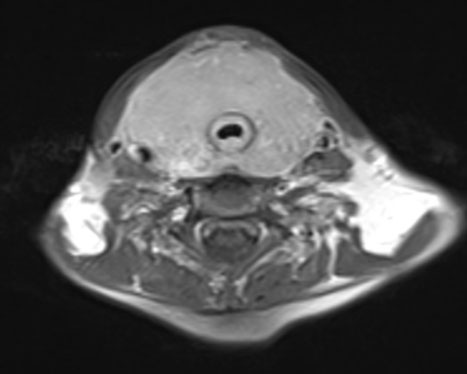
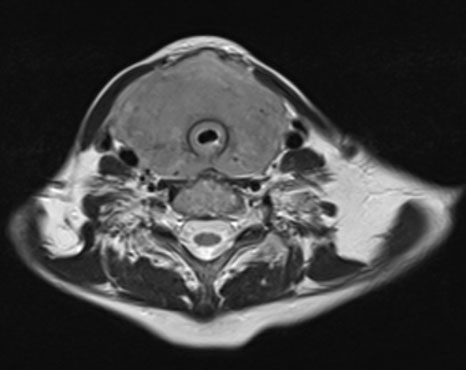
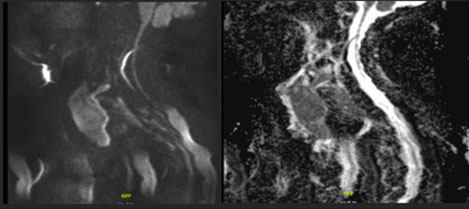
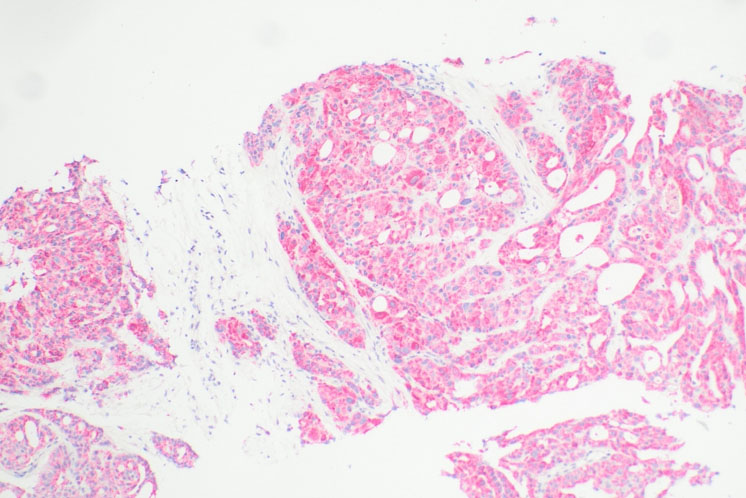
Fourteen years later, the patient presented to our institution with a palpable cervical mass. A total body CT revealed a non-enhancing diffusely enlarged hypodense thyroid gland without the presence of enlarged lymph nodes or other significant abnormalities (Figure 3). A magnetic resonance (MR) examination of the neck done one month later showed a rapid increase in size of the thyroid gland demonstrating diffuse enhancement postgadolinium administration and restricted diffusion. It showed to exert mass effect on the surrounding structures and significant narrowing of the airways. No pathological lymph nodes were seen (Figure 4, Figure 5, Figure 6). Because of the patient’s previous history of lymphoma and rapid growth of the thyroid gland, the possibility of extra-nodal thyroid lymphoma recurrence was raised, and a core needle biopsy of the thyroid gland was done and sent to pathology which confirmed the presence of diffuse large B-cell lymphoma within the thyroid gland.
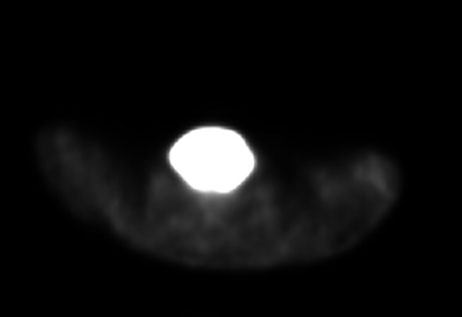
A whole-body PET-CT done revealed an intensely fluorodeoxyglucose (FDG) avid enlarged thyroid gland, reaching posteriorly to the prevertebral spaces and inferiorly to the retrosternal and upper paratracheal space without the presence of suspicious lymph nodes (Figure 7).

Discussion
A high index of clinical suspicion is required to make the diagnosis of primary thyroid lymphoma, notably in patients with a previous history of lymphoma presenting for rapid enlargement of the thyroid gland. Imaging modalities, notably magnetic resonance imaging (MRI) and PET-CT, are very useful when making the diagnosis and allows to evaluate the extent of the disease and the presence of nodal/metastatic disease. In this example, imaging showed a diffusely enlarged non-enhancing thyroid gland showing FDG avidity on PET-CT without nodal involvement or distant metastasis, supporting the evidence of a primary localized relapse. Similar cases of primary thyroid lymphoma have been reported previously, Benjelloun et al. described eight confirmed cases of primary thyroid lymphomas in patients who initially presented for a rapidly enlarging neck mass [5]. They were all treated with chemotherapy, particularly the rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) regiment, the mainstay treatment. The final diagnosis was confirmed by histopathology with core needle biopsy, which remain the gold standard for diagnosis.
Conclusion
This case demonstrates a rare occurrence of delayed extra-nodal recurrence of diffuse large B-cell lymphoma as an isolated thyroid mass more than a decade after the initial remission. The implication of this report is to highlight that the clinical and radiological presentation of an isolated lymphoma recurrence to the thyroid gland can be very similar to other systemic manifestation of a rapidly enlarging thyroid gland. Therefore, malignancy should be considered in the differential, especially in patients with a previous history of lymphoma.
REFERENCES
1.
Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, editors. Harrison’s principles of internal medicine. 19th ed. New York: McGraw-Hill Education; 2015.

2.
Li S, Young KH, Medeiros LJ. Diffuse large B-cell lymphoma. Pathology 2018;50(1):74–87. [CrossRef]
[Pubmed]
3.
Bligh MP, Borgaonkar JN, Burrell SC, MacDonald DA, Manos D. Spectrum of CT findings in thoracic extranodal non-Hodgkin lymphoma. Radiographics 2017;37(2):439–61. [CrossRef]
[Pubmed]
4.
Zucca E. Extranodal lymphoma: A reappraisal. Ann Oncol 2008;19 Suppl 4:iv77–80. [CrossRef]
[Pubmed]
5.
Benjelloun H, Rami M, Chehbouni M, Oulghoul O, Lakhdar Y, Rochdi Y, Raji A. Primary thyroid lymphomas: A decade of clinical experience through eight case reports. Sch J Med Case Rep 2025;13(5):911–6. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Michael Achram - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Joe Yazbek - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Michael Achram et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}