Case Report
Clinical case of a giant asymptomatic low-grade appendiceal mucinous neoplasm
1 Chief General Surgery Unit, Mater Olbia Hospital, Olbia, Italy; Dipartimento Scienze Mediche e chirurgiche, Fondazione Policlinico Universitario A. Gemelli, IRCCS di Roma, Largo Agostino Gemelli 8, 00168 Roma, Italy
Address correspondence to:
Alessandro Verbo
Chief General Surgery Unit, Mater Olbia Hospital, Olbia, Italy; Dipartimento Scienze Mediche e chirurgiche, Fondazione Policlinico Universitario A. Gemelli, IRCCS di Roma, Largo Agostino Gemelli 8, 00168 Roma,
Italy
Access full text article on other devices

Access PDF of article on other devices

Article ID: 100146Z10AV2025
doi: 10.5348/100146Z10AV2025CR
How to cite this article
Verbo A. Clinical case of a giant asymptomatic low-grade appendiceal mucinous neoplasm. J Case Rep Images Oncology 2025;11(1):33–36.ABSTRACT
Introduction: Low-grade appendiceal mucinous neoplasms (LAMNs) are rare tumors with nonspecific clinical features. Abdominal computed tomography (CT) is the primary diagnostic tool. Surgical resection is the standard treatment, requiring “en bloc” tumor removal to minimize the risk of rupture. Laparoscopic surgery is a safe and effective approach.
Case Report: A 74-year-old female patient was admitted for evaluation of a pelvic mass. Physical examination revealed a non-tender abdomen with a palpable pelvic mass. Imaging showed significant thickening and dilation of the appendix. Laparoscopic surgery confirmed LAMN. The patient recovered well with no complications at follow-up.
Conclusion: Low-grade appendiceal mucinous neoplasms are rare tumors with variable presentations. Abdominal CT and enteroscopy are crucial for diagnosis. Laparoscopic surgery offers a safe and effective treatment, ensuring favourable outcomes.
Introduction
Appendiceal mucinous neoplasms (AMNs) are rare and occur in less than 0.3% of appendectomy specimens and representing for approximately 1% of gastrointestinal tumors [1]. In 2016, the Peritoneal Surface Oncology Group International classified AMNs into four categories: low-grade appendiceal mucinous neoplasms (LAMNs), high-grade appendiceal mucinous neoplasms, mucinous adenocarcinomas, and goblet cell carcinoids [2]. Low-grade appendiceal mucinous neoplasms, the most common subtype, are defined by mucinous neoplasms with low-grade cytology and at least one of the following features: absence of muscularis mucosae, submucosal fibrosis, “pushing” infiltration (protruding or diverticular-like growth), undulating or flattened epithelial proliferation, appendiceal rupture, or the presence of mucinous cells or material outside the appendix [2]. Low-grade appendiceal mucinous neoplasms primarily affect adults, particularly females, and are often diagnosed incidentally during appendectomy [3].
Case Report
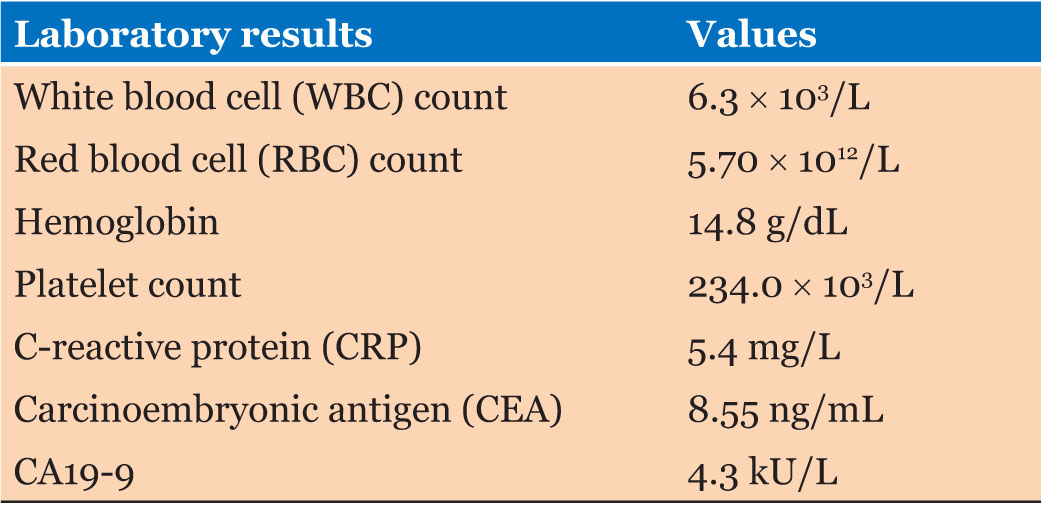
A 74-year-old female patient was admitted to our hospital due to a pelvic space-occupying lesion detected three months earlier. Clinical examination revealed a cystic lesion in the lower right abdomen. The patient denied symptoms such as fever, nausea, vomiting, abdominal pain, abdominal distension, hematemesis, or melena. The patient had a medical history of autoimmune hypothyroidism and previous surgeries for gallstones and a right ovarian cyst. She reported no history of smoking or alcohol consumption and had no significant family medical history. On admission, the patient was alert, oriented, and in good general condition. There were no signs of lymphadenopathy, and cardiovascular and pulmonary examinations were unremarkable. Abdominal examination revealed a soft, non-tender abdomen with a palpable mass in the lower right quadrant. Digital rectal examination confirmed the presence of a mass, but no other abnormalities were noted. Laboratory tests revealed the following:
Contrast-enhanced abdominal CT and MRI scans revealed significant thickening and dilation of the appendix (Figure 1 and Figure 2). Post-contrast imaging demonstrated slight enhancement of the appendiceal wall. Pathological analysis confirmed the presence of LAMN (Figure 3). Laparoscopic surgery was performed, revealing a markedly dilated appendix (Figure 4). A linear cutter/stapler was used to perform a laparoscopic ileocecal resection. The resected appendix measured 15 cm in length and 4 cm in width. Postoperative pathology confirmed tumor invasion throughout the appendix, with mucin accumulation observed in the apical portion and within the subserosal (SS) layer. The resection margins were negative for tumor involvement. The patient received symptomatic and supportive care, including nutritional therapy, without the need for antibiotic therapy. She was discharged on postoperative day 4 without complications such as abdominal bleeding, intestinal obstruction, or incision infection. During an outpatient follow-up in December 2024, routine blood tests, biochemical analyses, tumor marker assessments, and chest and abdominal CT scans revealed no evidence of recurrence.




Discussion
Diagnosing LAMNs is challenging due to their rarity, nonspecific clinical symptoms, and lack of specific tumor markers. The primary symptom is right lower quadrant abdominal pain due to appendiceal lumen distension in the early stages of tumor growth, often mimicking acute or chronic appendicitis [4],[5]. Additional symptoms may include weight loss, nausea, vomiting, anorexia, altered bowel habits, and complications such as intestinal obstruction, intussusception, gastrointestinal hemorrhage, ureteral compression, infections, or tumor-related necrosis or hemorrhage in severe cases [2],[6]. Approximately 25% of LAMN patients are asymptomatic, with the condition frequently detected during routine health evaluations or unrelated surgeries [7]. Tumor rupture is the most serious complication, as it can lead to pseudomyxoma peritonei (PMP), characterized by mucinous ascites and intraperitoneal tumor cell dissemination, resulting in significant morbidity and mortality [8]. Early diagnosis and intervention are critical to reduce the risk of PMP and improve outcomes. Imaging plays a pivotal role in diagnosing LAMNs. Ultrasound may reveal mucin accumulation and the “onion skin” sign, while CT scans are the most effective modality for identifying cystic dilation of the appendiceal lumen and irregular appendiceal wall thickening, often with calcifications [9]. Colonoscopy may demonstrate a smooth elevated mass at the appendiceal orifice, but visible mucinous tumors are rarely observed. The cornerstone of LAMN management is surgical resection to prevent rupture and the development of PMP. Complete tumor resection with negative margins is essential [10]. For localized tumors involving the distal appendix, appendectomy is typically sufficient. For extensive appendiceal involvement, especially near the base or cecum, partial cecum resection may be required. In cases of large or highly malignant tumors, ileocolic resection or right hemicolectomy may be necessary [11]. Laparoscopic surgery is the preferred approach due to its reduced surgical stress, decreased postoperative pain, and shorter recovery time. Studies, including those by Singh et al., have demonstrated that laparoscopic appendectomy using a specimen retrieval bag and low-pressure pneumoperitoneum is both safe and effective [12],[13]. Despite the risk of PMP, LAMNs’ slow progression and low malignant potential often result in favorable outcomes. Appendectomy or partial resection typically achieves negative margins and long-term disease control [14],[15],[16],[17].
Conclusion
Low-grade appendiceal mucinous neoplasms are rare tumors that often lack specific clinical manifestations and are typically identified incidentally during appendectomy. A thorough medical history and physical examination are essential before surgery. Abdominal CT and enteroscopy are critical diagnostic tools, while laparoscopic surgery is a safe and effective method for both diagnosis and treatment. Appendectomy or partial resection generally provides favorable outcomes, with the potential for a complete cure.
REFERENCES
1.
Galea LA, Acosta AM, Appu S. Low-grade mucinous lesion of the seminal vesicle: The counterpart of low-grade appendiceal mucinous neoplasm? Histopathology 2023;82(2):365–7. [CrossRef]
[Pubmed]

2.
Umetsu SE, Kakar S. Issues in assigning the T category in the staging of low-grade appendiceal mucinous neoplasm and high-grade appendiceal mucinous neoplasm. Arch Pathol Lab Med 2023;147(10):1107a–7. [CrossRef]
[Pubmed]
3.
Kurt E, Turanli S. How to manage localized low-grade appendiceal mucinous neoplasm? Cir Esp (Engl Ed) 2023;101(10):729–31. [CrossRef]
[Pubmed]
4.
Yao MQ, Jiang YP, Wang YY, Mou YP, Fan JX. Asymptomatic low-grade appendiceal mucinous neoplasm: A case report. World J Clin Cases 2024;12(2):361–6. [CrossRef]
[Pubmed]
5.
Boshnaq M, Toeima M, Hamade A, Bagla N. Local protocol for management of Low-Grade Appendiceal Mucinous Neoplasm (LAMN). Indian J Surg Oncol 2020;11(3):355–9. [CrossRef]
[Pubmed]
6.
Gonzalez HH, Herard K, Mijares MC. A rare case of low-grade appendiceal mucinous neoplasm: A case report. Cureus 2019;11(1):e3980. [CrossRef]
[Pubmed]
7.
Kwak HD, Ju JK. A prospective study of discrepancy between clinical and pathological diagnosis of appendiceal mucinous neoplasm. Ann Surg Treat Res 2020;98(3):124–9. [CrossRef]
[Pubmed]
8.
Yamaguchi T, Murata K, Shiota T, et al. Clinicopathological characteristics of low-grade appendiceal mucinous neoplasm. Dig Surg 2021;38(3):222–9. [CrossRef]
[Pubmed]
9.
Xiao J, Li P, Liu W. Analysis of clinical characteristics of Low-Grade Appendiceal Mucinous Neoplasm (LAMN): A retrospective cohort study of 51 LAMN patients. J Invest Surg 2021;34(7):721–7. [CrossRef]
[Pubmed]
10.
Wu YC, Wen L, Dou WD, Zhang JL, Wu T, Wang X. Clinicopathological analysis and surgical strategy of primary appendiceal neoplasms. [Article in Chinese]. Zhonghua Wei Chang Wai Ke Za Zhi 2021;24(12):1065–72. [CrossRef]
[Pubmed]
11.
Qi XM, Sun P, Wan JY. Clinicopathologic analysis of low appendiceal mucinous neoplasm. Zhonghua Quanke Yishi Zazhi 2016;15:871–4.
12.
Chicago Consensus Working Group. The Chicago consensus on peritoneal surface malignancies: Management of appendiceal neoplasms. Ann Surg Oncol 2020;27(6):1753–60. [CrossRef]
[Pubmed]
13.
Han S, Li XW, Zhao PX, Guan TW, Li SY, Zhang DJ. Research progress on the diagnosis and treatment of low-grade appendiceal mucinous neoplasm. Zhonghua Jiepouyulinchuang Zazhi 2019;24:512–5.
14.
Singh MK, Kumar MK, Singh R. Laparoscopic appendectomy for mucocele of the appendix. J Nat Sci Biol Med 2014;5(1):204–6. [CrossRef]
[Pubmed]
15.
Al-Tarakji M, Ali SM, Shah AA, Petkar MA, Mirza S, Singh R, et al. A unique case of low-grade mucinous neoplasm in stump appendectomy. Case Rep Surg 2020;2020:8850403. [CrossRef]
[Pubmed]
16.
Carr NJ, Cecil TD, Mohamed F, Sobin LH, Sugarbaker PH, González-Moreno S, et al. A consensus for classification and pathologic reporting of pseudomyxoma peritonei and associated appendiceal neoplasia: The results of the Peritoneal Surface Oncology Group International (PSOGI) modified delphi process. Am J Surg Pathol 2016;40(1):14–26. [CrossRef]
[Pubmed]
17.
Ramaswamy V. Pathology of mucinous appendiceal tumors and pseudomyxoma peritonei. Indian J Surg Oncol 2016;7(2):258–67. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Alessandro Verbo - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Data Availability StatementThe corresponding author is the guarantor of submission.
Consent For PublicationWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Competing InterestsAuthor declares no conflict of interest.
Copyright© 2025 Alessandro Verbo. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.